Review Article
 Download PDF (3.41 MB)
Download PDF (3.41 MB)
Journal of Structural Heart Disease, June 2017, Volume 3, Issue 3:62-72
DOI: 10.12945/j.jshd.2017.016.14
Transcatheter Pulmonary Valve Replacement
The Edwards Sapien Valve
Joseph DeGiovanni, MD, FRCP, FRCPCH
Department of Cardiology, Children’s & Queen Elizabeth Hospitals, Birmingham, UK
Abstract
Pulmonary valve replacement is one of the most common surgical procedures performed in older children and adults with congenital heart disease who have normally had at least one previous operation. The percutaneous alternative was first performed in man in 2000 when Dr. Bonhoeffer merged a surgically available bovine jugular vein valve (Venpro/Contegra) and a Cheatham-Platinum (CP) stent to create a percutaneous system for stenosed conduits; this valve was subsequently acquired by Medtronic and is now the Melody valve. The Edwards Sapien valve was originally designed for percutaneous aortic valve replacement (TAVI/TAVR), but its design makes it equally suitable for pulmonary implantation using a similar delivery system and it is indeed indicated for this purpose [1, 2]. The Edwards valve has evolved over recent years, increasing the range of sizes including the 29-mm Edwards XT and, more recently, the Sapien 53. The Edwards 3, incorporates a cuff/skirt outside of the frame to minimize paravalvular leaks; it was primarily designed for the aortic position where paravalvular leaks are generally more significant. Follow-up observations indicate that the performance and longevity of the Edwards percutaneous valve are comparable to surgically implanted bioprostheses which are also manufactured by Edwards Lifesciences; the catheter technique has reached a high level of sophistication to achieve successful and safe results in selected individuals. Some patients, however, would be better candidates for surgery, usually for anatomic reasons. Transcatheter pulmonary valve implantation has some advantages over surgery, as it is less invasive, avoids repeat sternotomy and bypass, does not usually require intensive care, and results in a shorter hospital stay. Cost effectiveness is comparable, and because the Edwards valve is based on a well-established tissue valve technology, its longevity are performance are expected to be similar to that of surgery as the frame on which the valve is mounted is very robust with complete integrity maintained over at least 5 years from implantation.
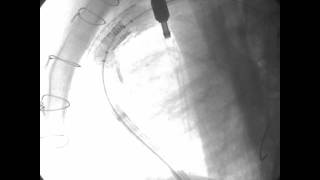
Video 1

Panel A. Sequence of angiograms in wide RVOT pre-stent, following two stents and a SAPIEN XT. Courtesy Dr. Mansour Aljufan.
Video 2

Panel B. Sequence of angiograms in wide RVOT pre-stent, following two stents and a SAPIEN XT. Courtesy Dr. Mansour Aljufan.
Video 3

Panel C. Sequence of angiograms in wide RVOT pre-stent, following two stents and a SAPIEN XT. Courtesy Dr. Mansour Aljufan.
Video 4

Panel D. Sequence of angiograms in wide RVOT pre-stent, following two stents and a SAPIEN XT. Courtesy Dr. Mansour Aljufan.
Video 5

Panel E. Sequence of angiograms in wide RVOT pre-stent, following two stents and a SAPIEN XT. Courtesy Dr. Mansour Aljufan.
Video 6

Note slow balloon inflation and fine tuning of valve position to landing zone. Balloon bursts at full inflation but valve is fully deployed and stable.
Video 7
Note circular Edwards valve configuration for optimal function.
Cite this article as: DeGiovanni J. Transcatheter Pulmonary Valve Replacement – The Edwards Sapien Valve. Structural Heart Disease 2017;3(3):62-72. DOI: 10.12945/j.jshd.2017.016.14
All comments will be screened and reviewed before posting. Statements, opinions, and results of studies published in Journal of Structural Heart Disease are those of the authors and do not reflect the policy or position of The Journal and Science International and the Editorial Board and provides no warranty as to their accuracy or reliability. Material is copyrighted and owned by Science International and cannot be used without expressed permission.
Review Article
Journal of Structural Heart Disease, June 2017, Volume 3, Issue 3:62-72
DOI: 10.12945/j.jshd.2017.016.14
Transcatheter Pulmonary Valve Replacement
The Edwards Sapien Valve
Joseph DeGiovanni, MD, FRCP, FRCPCH
Department of Cardiology, Children’s & Queen Elizabeth Hospitals, Birmingham, UK
Abstract
Pulmonary valve replacement is one of the most common surgical procedures performed in older children and adults with congenital heart disease who have normally had at least one previous operation. The percutaneous alternative was first performed in man in 2000 when Dr. Bonhoeffer merged a surgically available bovine jugular vein valve (Venpro/Contegra) and a Cheatham-Platinum (CP) stent to create a percutaneous system for stenosed conduits; this valve was subsequently acquired by Medtronic and is now the Melody valve. The Edwards Sapien valve was originally designed for percutaneous aortic valve replacement (TAVI/TAVR), but its design makes it equally suitable for pulmonary implantation using a similar delivery system and it is indeed indicated for this purpose [1, 2]. The Edwards valve has evolved over recent years, increasing the range of sizes including the 29-mm Edwards XT and, more recently, the Sapien 53. The Edwards 3, incorporates a cuff/skirt outside of the frame to minimize paravalvular leaks; it was primarily designed for the aortic position where paravalvular leaks are generally more significant. Follow-up observations indicate that the performance and longevity of the Edwards percutaneous valve are comparable to surgically implanted bioprostheses which are also manufactured by Edwards Lifesciences; the catheter technique has reached a high level of sophistication to achieve successful and safe results in selected individuals. Some patients, however, would be better candidates for surgery, usually for anatomic reasons. Transcatheter pulmonary valve implantation has some advantages over surgery, as it is less invasive, avoids repeat sternotomy and bypass, does not usually require intensive care, and results in a shorter hospital stay. Cost effectiveness is comparable, and because the Edwards valve is based on a well-established tissue valve technology, its longevity are performance are expected to be similar to that of surgery as the frame on which the valve is mounted is very robust with complete integrity maintained over at least 5 years from implantation.
Supplemental Media
Video 1
Video 2
Video 3
Video 4
Video 5
Video 6
Video 7
PDF
Mobile-ready Flipbook
Cite this article as: DeGiovanni J. Transcatheter Pulmonary Valve Replacement – The Edwards Sapien Valve. Structural Heart Disease 2017;3(3):62-72. DOI: 10.12945/j.jshd.2017.016.14
You must be registered and logged in to leave comments.
There have been no comments posted yet
Ask a question (publicly)
Board